Our Goal
We're revolutionizing healthcare with AI that thinks, learns, and optimizes risk adjustment for better patient outcomes and organizational success.


Risk adjustment AI is only as good as the data behind it.
Health Data Max normalizes fragmented claims, charts, and encounter files into a clean, unified foundation — so every insight, submission, and audit is built on data you can trust.
CMS is moving from a handful of audits a year to all eligible MA contracts — across six open payment years. Health Data Max keeps your submissions continuously audit-ready.
Risk Adjustment Data Validation is how CMS checks whether the diagnoses an MA plan submitted for payment are actually supported in the member's medical record.
CMS pays MA organizations a risk-adjusted amount for each enrollee. Diagnoses submitted by providers map to Hierarchical Condition Categories (HCCs), each carrying a factor that raises the member's risk score — and the monthly payment to the plan.
Because payment follows diagnosis, CMS validates a sample of those diagnoses against the underlying charts. In a RADV audit, the plan must produce a medical record that supports each sampled HCC. If the record doesn't support the diagnosis, the HCC is invalidated, the risk score is overstated, and the associated payment is recovered.
CMS can then extrapolate the sampled error across the contract's full sampling frame, turning a modest sample into a large recovery. The 2023 rule that authorized extrapolation (and removed the fee-for-service adjuster) was vacated by a federal court in 2025 and is under appeal — but CMS has expressly designed its PY2020 and PY2021 audits to support extrapolated recoveries and reserves the right to collect them if legally permissible. Plan for extrapolation; don't bank on the litigation.
On May 21, 2025, CMS announced an aggressive strategy to enhance and accelerate MA audits — clearing the backlog and auditing everyone.
CMS will audit all eligible MA contracts each year in newly initiated audits — roughly a 900% increase in audit volume, reaching nearly every contract.
Sample size scales with contract size (200 / 100 / 50 / 35 by stratum), and members aren't picked at random — CMS targets the enrollees its improper-payment model predicts will lose the most risk score.
CMS expanded its coder workforce from ~40 to ~2,000 and is using AI-assisted review to clear years of open audits on a compressed timeline — though final overpayment determinations stay with human coders.
CMS's PY2020 and PY2021 Audit Methods & Instructions lay out the full mechanics — from how members are selected to how overpayments are calculated and extrapolated.
It starts before you know it. CMS defines a sampling frame, draws a statistically valid random sample, and sends an Audit Notice to your CEO, CFO, COO, and Compliance Officer. Your team designates points of contact, registers in CMS's secure CDAT portal, and downloads the Enrollee Data List (EDL) naming the exact enrollees, HCCs, and diagnosis codes under review.
From there the clock runs hard: pull a valid medical record — legibly signed and dated, from a face-to-face visit by a credentialed provider, within the data collection year — for every audited HCC, and submit it through CDAT before the deadline. CMS coders then abstract diagnoses through up to three rounds of review and classify each HCC as Confirmed, Confirmed Higher, Discrepant, Discrepant Lower, or Administrative Exception.
The sample isn't random across your whole book. CMS first ranks audit-eligible enrollees — broadly, those enrolled for all 12 months of the data-collection year and at least one month of the payment year — with a "predicted improper payment" model, then samples from the top quartile most likely to lose risk score under review. The exact formula isn't published, but it's expected to lean on circumstantial coding-risk signals:
// These are the exact OIG high-risk signatures below — acute Dx with no inpatient claim, cancer with no treatment, embolism with no anticoagulant. The audit target and the OIG pattern are the same thing.
CMS sorts RADV-eligible contracts by sampling-frame size into four strata. The ten largest contracts draw the deepest samples — which is exactly why our data shows audit probability rising with enrollment.
The month CMS plans to begin RADV audits, by MA payment year. Six payment years are now on the calendar.
HHS-OIG built a public toolkit from its MA audits, identifying diagnosis codes that — when paired with other data — are at high risk of being unsupported. The error rates are striking.
Across its audits, OIG found that roughly 70% of the high-risk diagnosis codes it reviewed were not supported by the associated medical records — and within specific groups, error rates exceeded 90%. These aren't edge cases; they're patterns a plan can detect and correct before CMS arrives.
| High-Risk Group | Records in Scope | Errors | Error Rate |
|---|---|---|---|
| Acute stroke | 945 | 908 | 96% |
| Acute heart attack | 791 | 751 | 95% |
| Embolism | 754 | 593 | 79% |
| Lung cancer | 391 | 345 | 88% |
| Breast cancer | 390 | 373 | 96% |
| Colon cancer | 390 | 368 | 94% |
| Prostate cancer | 360 | 322 | 89% |
| Potentially mis-keyed codes | 522 | 421 | 81% |
| Totals | 4,543 | 4,081 | 90% |
Source: HHS-OIG, "Toolkit To Help Decrease Improper Payments in Medicare Advantage Through the Identification of High-Risk Diagnosis Codes" (Dec 2023, A-07-23-01213), errors as of Nov 2023.
Each high-risk group follows a recognizable signature: an acute diagnosis submitted without the clinical evidence you'd expect to accompany it. In most cases, a "history of" code — which doesn't map to an HCC — was what the record actually supported.
One acute stroke diagnosis on a physician claim, with no matching inpatient or outpatient hospital claim.
An acute MI on a single physician/outpatient claim with no inpatient claim within 60 days before or after.
An embolism diagnosis with no anticoagulant medication dispensed — the treatment you'd expect for an active embolism.
A lung cancer diagnosis with no surgery, radiation, or chemotherapy within six months before or after.
A breast cancer diagnosis without surgical, radiation, chemotherapy, or relevant drug treatment in the window.
A colon cancer diagnosis with no surgical therapy, radiation, or chemotherapy in the six-month window.
A prostate cancer diagnosis in members 74 or younger with no treatment evidence in the surrounding window.
A single transposed or mistyped code (e.g., I720 → I270) that mapped to an unrelated, unvalidated HCC.
HDM doesn't wait for an Audit Notice. Provider claims, encounters, CMS response files, payment and risk-score data, and chart coding all live in one database — so every submitted diagnosis stays continuously linked to the record that has to support it. When CMS initiates on its new accelerated timeline, you're already prepared instead of scrambling inside a four-month window.
Claims, encounters, CMS response files, risk scores, payments, and chart coding — reconciled and member-linked in a single source of truth.
→Mirror CMS's improper-payment signals and OIG high-risk logic — single-encounter HCCs, chart-review-only adds, thin utilization — before they're ever sampled.
→Plans upload medical records; HDM surfaces the strongest supporting chart for each suspect member-HCC.
→Confirm defensible HCCs, and route truly unsupported diagnoses for correction — accurate payment, clean record.
With PY2020–PY2025 on the CMS schedule, the question isn't whether your plan will be audited — it's whether your records are ready. Let's review your highest-risk HCCs together.
Program rules, audit workflow, sampling logic, medical record standards, business rules, and deadlines for BY2024 and BY2025 — in one place.
HHS Risk Adjustment Data Validation (HHS-RADV) is CMS's annual audit program that verifies the accuracy of the diagnoses issuers submit to the EDGE server — the same diagnoses that drive risk scores and determine how much each issuer receives or pays through ACA Risk Adjustment.
Risk adjustment redistributes funds among issuers in the same state market risk pool based on relative member health risk. Issuers with sicker-than-average enrollees receive transfers; those with healthier-than-average enrollees pay charges. RADV audits the data quality behind those transfers.
Because payment follows diagnosis, CMS validates a sample of those diagnoses against the underlying medical records. An unsupported HCC fails, the issuer's Plan Liability Risk Score (PLRS) is adjusted, and RADV-adjusted RA transfers are applied.
All non-grandfathered, non-transitional plans. Issuers in states with more than one issuer in the risk pool are subject to sampling.
An issuer with a high Super HCC failure rate in any of 3 Failure Rate Groups may qualify as an outlier — triggering an error rate adjustment to their PLRS for that benefit year.
EDGE data locked April 30 → RA cycle closes ~May → sample drawn ~Jun–Jul → IVA packages due ~Jan of the following year → final results ~Jun. Accuracy during submission time determines audit outcome.
The issuer selects a CMS-approved IVA Entity to review medical records for each of the 200 sampled enrollees. The IVA Entity validates D&E data, RXC categories, and every EDGE-submitted HCC against source documentation — submitting findings via the CMS RADV Audit Tool.
A single CMS-designated SVA Entity independently re-abstracts a subsample of IVA records with no access to IVA findings. The pairwise means test determines whether IVA or SVA results feed error estimation. Subsamples expand automatically if precision is insufficient.
Non-grandfathered individual and small group (including merged) market risk adjustment covered plans, inside and outside the Exchange.
45 CFR §§ 153.350, 153.630. Mandated under the ACA; implemented through annual CMS Payment Notice rulemaking.
HHS-HCC Version 08 (V08). Mappings and coefficients published in the 2026 Payment Notice (90 FR 4424).
HDM doesn't wait for the RADVIVAS reports to land. EDGE submissions, accepted claims, RA outputs, and source enrollment are reconciled in one database — so every HCC is traceable to the chart that has to support it before CMS samples.
Accuracy in both directions. The goal isn't to maximize codes — it's to make every submitted HCC defensible. HDM flags potential over-coding and unsupported diagnoses for correction just as it surfaces supporting evidence, so your risk capture is accurate, compliant, and able to withstand the SVA's independent re-review.
With BY2024 audits active and BY2025 on the calendar, the window to get ahead of your IVA cycle is now.
Program rules, audit workflow, sampling logic, medical record standards, business rules, and deadlines for BY2024 and BY2025 — in one place.
CMS's annual audit program that verifies the diagnoses issuers submit to the EDGE server are actually supported by medical records.
HHS Risk Adjustment Data Validation (HHS-RADV) is CMS's annual audit program that verifies the accuracy of the diagnoses issuers submit to the EDGE server — the same diagnoses that drive risk scores and determine how much each issuer receives or pays through ACA Risk Adjustment.
Risk adjustment redistributes funds among issuers in the same state market risk pool based on relative member health risk. Issuers with sicker-than-average enrollees receive transfers; those with healthier-than-average enrollees pay charges. RADV audits the data quality behind those transfers.
Because payment follows diagnosis, CMS validates a sample of those diagnoses against the underlying medical records. An unsupported HCC fails, the issuer's Plan Liability Risk Score (PLRS) is adjusted, and RADV-adjusted RA transfers are applied.
RADV isn't a periodic spot-check — it's a structural part of every issuer's annual RA settlement.
Non-grandfathered individual and small group (including merged) market RA-covered plans, inside and outside the Exchange, in states where HHS operates risk adjustment.
An issuer with a high Super HCC failure rate in any of 3 Failure Rate Groups may qualify as an outlier — triggering an error rate adjustment to PLRS for that benefit year.
EDGE data locked April 30 → RA cycle closes ~May → sample drawn ~Jun–Jul → IVA packages due ~Jan of the following year → final results ~Jun. Submission-time accuracy decides audit outcome.
Two separate entities review the same enrollees — one contracted by the issuer, one contracted by CMS — and their results are statistically reconciled.
The issuer selects a CMS-approved IVA Entity to review medical records for each of the 200 sampled enrollees. The IVA Entity validates D&E data, RXC categories, and every EDGE-submitted HCC against source documentation, submitting findings via the CMS RADV Audit Tool.
A single CMS-designated SVA Entity independently re-abstracts a subsample of IVA records with no access to IVA findings. The pairwise means test determines whether IVA or SVA results feed error estimation.
Non-grandfathered individual and small group (including merged) market risk adjustment covered plans, inside and outside the Exchange.
45 CFR §§ 153.350, 153.630. Mandated under the ACA; implemented through annual CMS Payment Notice rulemaking.
HHS-HCC Version 08 (V08). Mappings and coefficients published in the 2026 Payment Notice (90 FR 4424).
The RADV lifecycle spans ~18–24 months from the benefit year's EDGE data cutoff to the final adjusted transfer. EDGE accuracy during the benefit year is what determines audit outcomes — the RADV command audits data that was locked months earlier.
The RADV sample is drawn from data already locked on the EDGE server. By the time a RADVIVAS report lands, an issuer has no ability to correct the underlying submission. Continuous EDGE data quality monitoring during the benefit year is the only effective RADV preparation.
The IVA sample is not a random draw from an issuer's full enrollment — CMS uses Neyman Allocation, a stratified sampling method.
CMS uses Neyman Allocation — a stratified sampling method that allocates sample size proportional to each stratum's share of the issuer population weighted by risk score variability.
For BY2025 and forward, Stratum 10 (enrollees with no HCCs) is excluded per 90 FR 4424. If a state risk pool has ≤200 HCC-bearing enrollees, all are selected — the full eligible population becomes the IVA sample.
*CMS first selects a 100-enrollee SVA subsample from the IVA-200, representative by stratum. SVA review then proceeds incrementally: 24 → 50 → full 100. Bootstrap pairwise means test (K=10,000, 90% CI) determines if results are accepted at each level. If SVA-100 precision is still poor, CMS expands to the full 200 (the entire IVA sample).
If issuer's total eligible population (≥1 HCC) is ≤200, all are selected. Allocation is proportional to stratum size × risk score variability via the Neyman formula.
Five steps turn medical record findings into a PLRS adjustment for outlier issuers.
Source: BY2025 HHS-RADV Protocols §10.4
Each HCC on the RADVDE Report must be supported by a qualifying medical record linked to an RA-eligible claim. The IVA Entity submits records through the Audit Tool; the SVA Entity re-abstracts the same records independently.
The ICD-10-CM code year applicable to the benefit year's date of service governs validity. Codes must be valid in the code set for the DOS.
BY2025 uses HHS-HCC V08. A diagnosis must map to an active HCC in V08 to contribute to PLRS. Mappings are in the Payment Notice.
The record must show the condition was assessed, monitored, or managed during the encounter — not merely listed in history.
Records from outside the benefit year cannot support a RADV HCC. Encounter date must fall within benefit year dates.
Diagnosing provider must hold credentials authorizing diagnosis in the state of practice. Scope-of-practice mismatches fail the HCC.
ICD-10 codes must be coded to highest available specificity. Unspecified codes where a specific alternative exists are subject to rejection.
Extracted from BY2025 HHS-RADV Protocols, BY2024 Package submission guidance, EDGE Business Rules, and IRR documentation. Click any rule to expand source citation.
April 30 is the last date for any claim submission or correction counting toward the RA calculation. After this date, the benefit year's data is locked. Enrollment files use full replacement; claims are incremental. EDGE data must be retained for 10 years (min. 3 years on active server).
| Date | Milestone | Responsible Party |
|---|---|---|
| Nov 2025 | Audit Tool opens for IVA Audit Results Submission | IVA Entity |
| Jan 8, 2026 | Package 1 submission deadline (8:00 PM ET) | IVA Entity |
| Jan 15, 2026 | Package 2 submission deadline + IRR submission due | IVA Entity |
| Jan–Mar 2026 | SVA review window | SVA Entity |
| Mar 2026 | Summary of Final Pairwise Results released | CMS |
| +15 days | Discrepancy Window 1 (insufficient pairwise agreement only) | Issuers |
| Jun 2026 | Final Results Memo published | CMS |
| +30 days | Error Rate Discrepancy Window 2 | Issuers |
| Date | Milestone | Responsible Party |
|---|---|---|
| Apr 13, 2026 | BY2025 IVA Entity Designation Web Form opens | Issuers |
| Apr 30, 2026 | EDGE data cutoff — last day for claim corrections | Issuers |
| Nov 2026 | Audit Tool opens for IVA Audit Results Submission | IVA Entity |
| Jan 7, 2027 | Package 1 submission deadline (8:00 PM ET) | IVA Entity |
| Jan 14, 2027 | Package 2 submission deadline + IRR submission due | IVA Entity |
| Jan–Mar 2027 | SVA review window | SVA Entity |
| Mar 2027 | Summary of Final Pairwise Results released | CMS |
| +15 days | Discrepancy Window 1 (insufficient pairwise agreement only) | Issuers |
| Jun 2027 (est.) | Final Results Memo (based on BY2024 pattern) | CMS |
| +30 days | Error Rate Discrepancy Window 2 | Issuers |
Est. = estimated based on BY2024 pattern. Source: 2025 BY HHS-RADV Activities Timeline; BY2025 Issuer Participation Slides (Mar 2026).
All terms extracted from BY2025 HHS-RADV Protocols, EDGE Business Rules, IRR guidance, and CMS REGTAP materials.
HDM doesn't wait for the RADVIVAS reports to land. EDGE submissions, accepted claims, RA outputs, and source enrollment are reconciled in one database — so every HCC is traceable to the chart that has to support it before CMS samples.
Enrollment, claims, RA outputs, and RADV reports linked per issuer and benefit year.
→Mirror Super HCC failure rate signals and D&E/RXC anomaly patterns before the sample drops.
→For each sampled enrollee-HCC, surface the strongest linked medical record and claim chain.
→Confirm defensible HCCs, route unsupported diagnoses for correction — accurate RA transfer.
With BY2024 audits active and BY2025 on the calendar, the window to get ahead of your IVA cycle is now.
Powered by Agentic AI & Fine-Tuned LLMs
Every Health Data Max solution leverage Agentic AI—a multi-agent intelligence architecture designed to continuously review CMS files, member charts, and claims data. Each product, from chart review to RADV defense, benefits from these agents’ ability to reason, validate, and adapt to changing CMS models.
This ensures unmatched accuracy, auditability, and compliance across your risk adjustment lifecycle.
Delivering real-time clinical intelligence at the chart level
Leverages proprietary NLP and LLMs to scan structured & unstructured data for HCCs and missed coding opportunities.
Assists coders and QA teams with compliant code suggestions, source-linked references, and confidence scoring.
Supports prospective, retrospective, and concurrent chart reviews.
Tracks every action for audit-readiness and traceability (full audit trail).
Seamlessly integrates with your existing EHR or coding platform.
Automated validation and reconciliation across your entire submission pipeline
Ingests and analyses X12 837 I/P/D encounter files.
Monitors TA1, 999, 277CA, MAO-002, MAO-004, MMR, and MOR files for errors and rejection trends.
Real-time dashboards flag rejected or dropped encounters.
Built-in reconciliation tools link rejected claims to charts, ensuring no revenue is lost.
Keeps your plan audit-ready and aligned with CMS requirements.
Automated validation and reconciliation across your entire submission pipeline
Drive more accurate risk scoring and maximize revenue without over-coding
Identifies undocumented HCCs across clinical records using AI.
Prioritizes high-impact, high-chronic patients to close the right gaps first.
Supports prospective programs that improve performance before the look-back ends.
Reduces risk of over- or under-coding by flagging anomalies with contextual evidence.
Generates predictive RAF impact and submission completeness metrics.
Drive more accurate risk scoring and maximize revenue without over-coding

Agentic AI in Healthcare
Transform Risk Adjustment with AI That Actually Works
Cut chart review time by 80% and boost RAF scores helped by AI agents that think, learn, and optimize your entire risk adjustment workflow.
We're revolutionizing healthcare with AI that thinks, learns, and optimizes risk adjustment for better patient outcomes and organizational success.
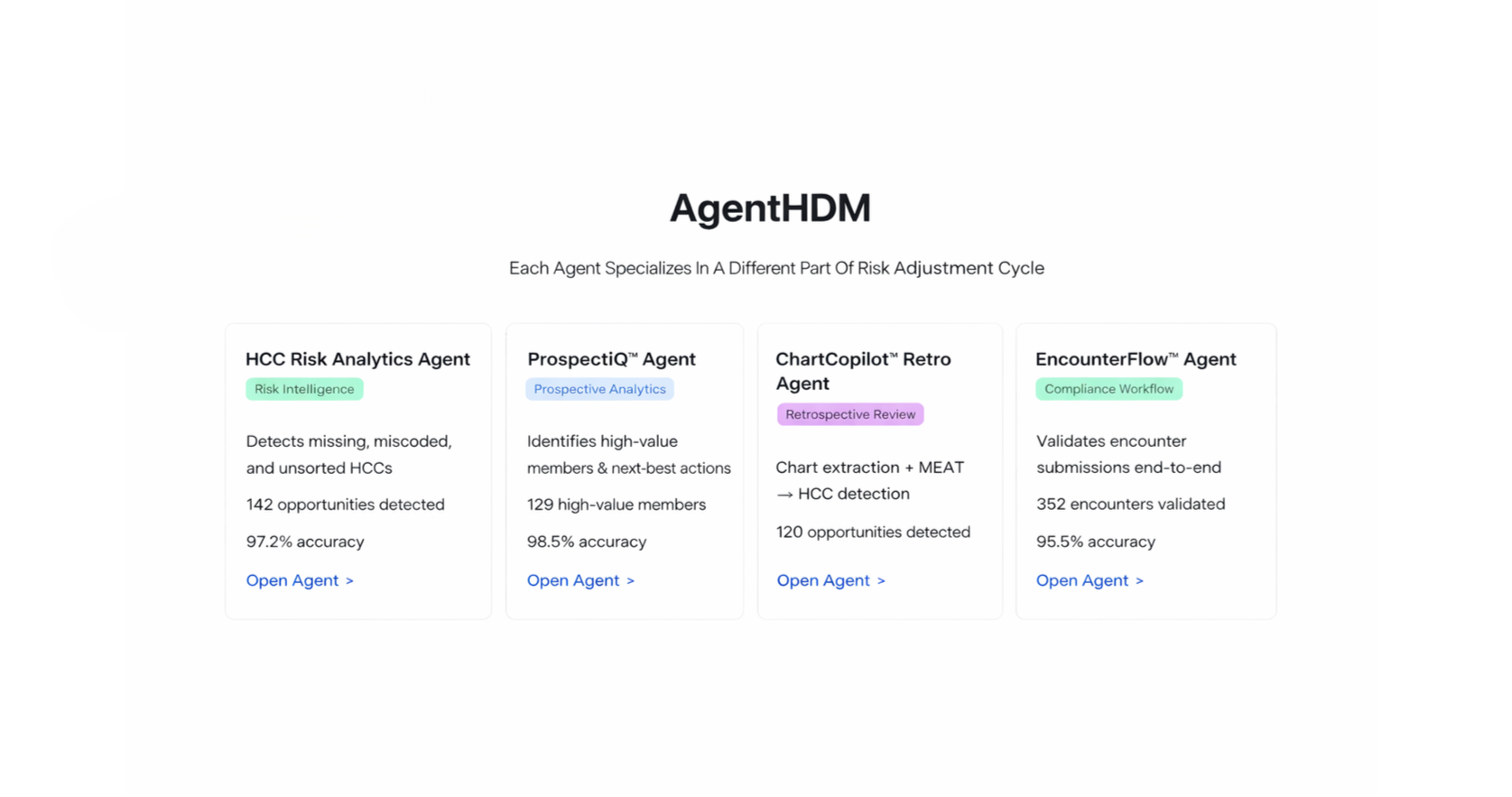
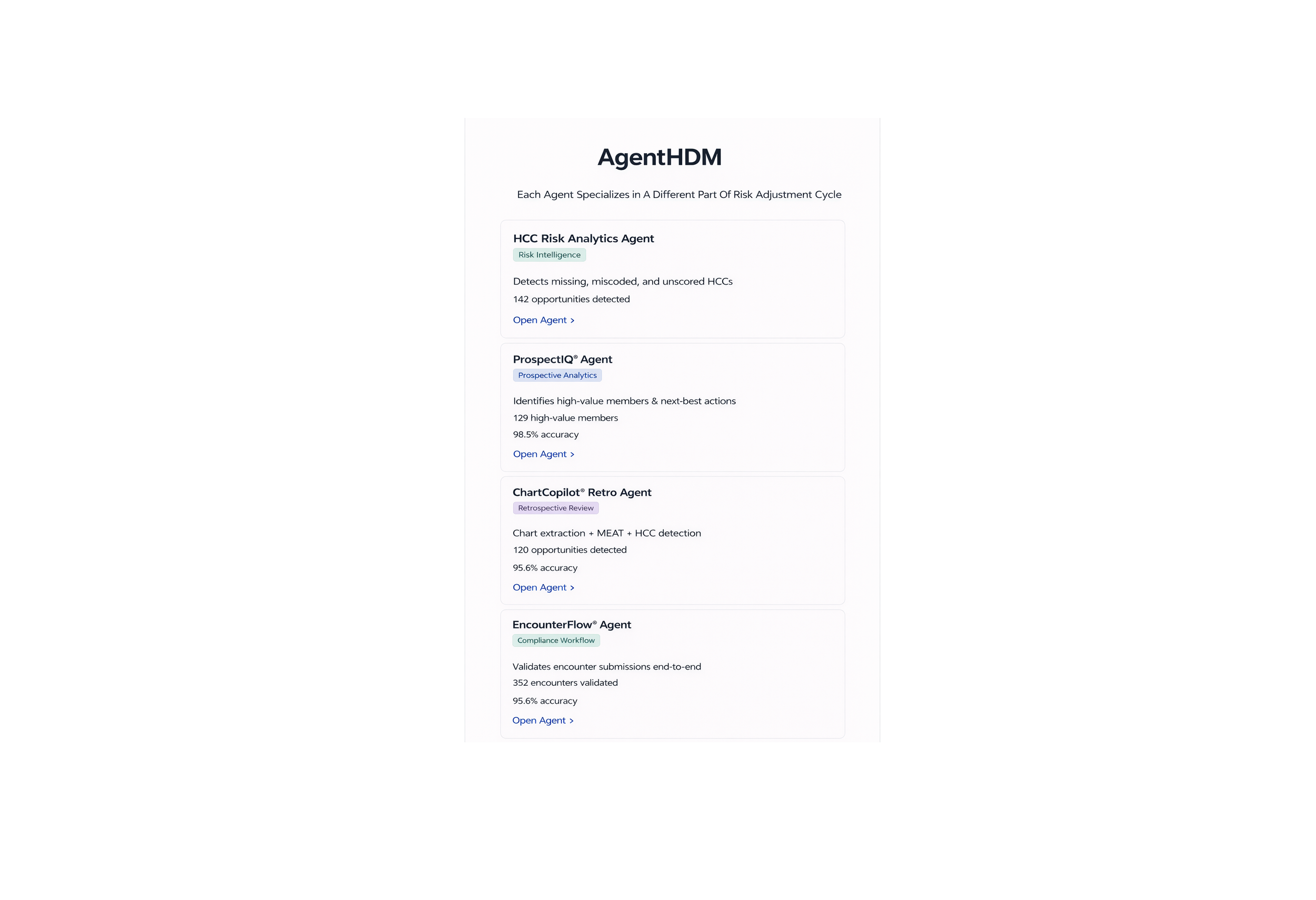
From identifying missed HCCs to validating encounters before submission, AgentHDM agents turn fragmented workflows into a single, intelligent operating layer — reducing rework, improving accuracy, and strengthening compliance.
Each AgentHDM agent is engineered as a purpose-specific decision system — not a generic AI assistant. While agents share a common intelligence layer, their capabilities are tightly scoped to the function they perform, ensuring consistent behavior across analytics, chart review, and submission workflows.
Agents combine deterministic logic (CMS guidance, HCC hierarchies, and submission rules) with statistical models trained on historical claims, encounters, and chart data. This hybrid approach allows the system to produce explainable outputs — showing what was identified, how it was evaluated, and which evidence supports the result.
Rather than acting autonomously on source systems, agents generate structured, traceable outputs designed for downstream use by analysts, coders, and operations teams — enabling review, validation, and confident execution at scale.
AgentHDM agents connect chart review, analytics, and submission into one intelligent operating layer — reducing rework, improving accuracy, and strengthening compliance.
Each agent is purpose-built, not generic. Shared intelligence ensures consistency, while tightly scoped roles keep behavior predictable across workflows.
By combining CMS rules and HCC logic with models trained on historical data, agents deliver explainable, evidence-backed outputs — showing what was found, why it matters, and how it was validated.
Outputs are structured for human review, enabling analysts and coders to act with confidence — not blind automation.
AI-powered chart reviews using your historical Medicare Advantage data run up to 80% faster by auto-summarizing clinical evidence, flagging suspected HCC gaps, and pre-building reviewer-ready findings. Reviewers spend less time searching across claims and encounters and more time validating what matters—driving faster throughput, recapture, and submissions without compromising compliance.
AI chart reviews achieve 98% accuracy through cross-validation against Medicare Advantage history. Each diagnosis is validated with MEAT evidence and checked for consistency across prior claims, encounters, and MAO-004/MMR/MOR signals, reducing false positives and rework. Clear, traceable rationales ensure consistent decisions, cleaner coding, and stronger RADV readiness.
Always-on AI chart review processing runs 24/7, including nights and weekends. As charts arrive, the system continuously triages, prioritizes, and routes evidence-backed opportunities with next-best actions. Teams start each day with the highest-impact work already queued—no downtime, no backlog spikes, just continuous progress toward compliant risk capture.
Our autonomous agents work together to revolutionize every step of your risk adjustment process
AI automatically processes medical records, EMR data, and claims across all formats. No manual data entry required.
Advanced NLP identifies HCC opportunities with 99.8% accuracy. Our AI learns from every interaction to improve continuously.
Built-in RADV audit protection ensures every code meets CMS requirements. Automated compliance checking prevents costly errors.
Streamlined submission process with real-time tracking. Get paid faster with error-free claims and comprehensive audit trails.
Complete AI-Powered Solutions
Everything you need for end-to-end risk adjustment automation
Powered by Agentic AI, Health Data Max connects every function—analytics, documentation, validation, and audit—through one autonomous, governed system
Powered by Agentic AI, Health Data Max connects every function—analytics, documentation, validation, and audit—through one autonomous, governed system
Powered by Agentic AI, Health Data Max connects every function—analytics, documentation, validation, and audit—through one autonomous, governed system
Detects missing, miscoded, and unsorted HCCs
97.2% accuracy
Identifies high-value members & next-best actions
98.5% accuracy
Chart extraction + MEAT → HCC detection
120 opportunities
Validates encounter submissions end-to-end
95.5% accuracy
Agentic AI in Healthcare
Transform Risk Adjustment with AI That Actually Works
Cut chart review time by 80% and boost RAF scores with autonomous AI agents that think, learn, and optimize your entire risk adjustment workflow.
Our autonomous agents work together to revolutionize every step of your risk adjustment process
AI ingests records and claims—no manual work
NLP identifies HCCs with 99.8% accuracy
RADV-ready compliance checks built in
Faster, cleaner submissions with full audit trails